Menopause Belly Fat: Why It Happens & How to Fight It
Menopause belly fat has multiple causes — hormones, sleep, stress & medications. Learn why it happens and evidence-based ways to fight it.


If you've noticed your waistline expanding in your 40s or 50s, you're not imagining it. Menopause belly fat is one of the most common — and most frustrating — changes women experience during the menopause transition. But understanding why it happens is the first step toward doing something about it.
According to Jean Marino, CNP, a menopause specialist at University Hospitals, "the number one reason for increased belly fat is a decrease in physical activity, but for women in the menopause transition, there are almost always other factors at play." Those factors include hormonal shifts, disrupted sleep, rising stress levels, and even certain medications.
This article breaks down each of those causes and — critically — what you can actually do about them.

Why Menopause Triggers Belly Fat: The Hormonal Story
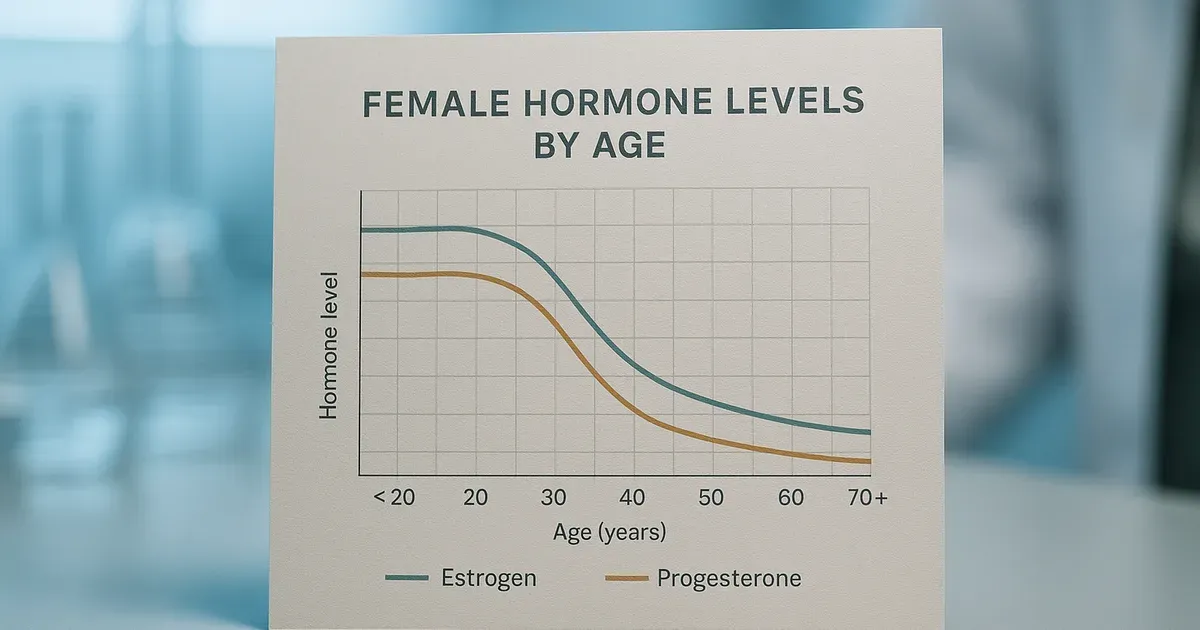
Hormonal change is at the heart of menopause belly fat, and the mechanics are more complex than most people realise. During perimenopause and menopause, estrogen and progesterone — two hormones that work in tandem throughout the reproductive years — begin to decline sharply. That drop doesn't happen in isolation; it sets off a hormonal chain reaction.
Testosterone Becomes More Available
Most people don't associate testosterone with women's bodies, but the ovaries and adrenal glands produce it in small amounts throughout a woman's life. When estrogen falls, the relative proportion of available testosterone rises. This hormonal imbalance can trigger a redistribution of body fat — shifting it away from the hips and thighs and toward the abdomen.
This is why the classic "pear-shaped" fat distribution of younger women can give way to a more "apple-shaped" profile during and after menopause.
Hunger Hormones Go Out of Balance
Estrogen plays a quiet but important role in appetite regulation. Lower estrogen levels cause a drop in leptin, a hormone that naturally suppresses appetite. At the same time, poor sleep — itself a hallmark of the menopause transition — causes ghrelin levels to rise. Ghrelin signals hunger and encourages the body to hold onto excess weight.
The result: you feel hungrier, feel less satisfied after eating, and your body is primed to store calories rather than burn them.
Sleep Disruption, Stress, and the Belly Fat Connection
Menopause belly fat isn't only a hormone story — it's also a lifestyle story, and two of the biggest lifestyle drivers are disrupted sleep and elevated stress.
Why Sleep Matters So Much
Lower estrogen, combined with common mood disorders like anxiety and depression, makes quality sleep harder to come by during menopause. It can become difficult to fall asleep or stay asleep, and the risk of sleep apnea increases. Women who are sleep-deprived have less energy for physical activity the next day and are significantly more likely to reach for comfort foods — particularly simple carbohydrates — that promote fat storage.
This creates a self-reinforcing cycle: poor sleep leads to weight gain, which can worsen sleep apnea, which leads to worse sleep.
The Stress-Weight Gain Spiral
Perimenopause and menopause bring a heightened risk of mood changes, particularly for women with a prior history of anxiety, depression, PMS, or postpartum depression. These mood shifts can manifest as fatigue, feeling overwhelmed, or lowered self-esteem — all of which can alter eating habits.
Beyond internal hormonal stress, many women at this stage of life are simultaneously managing major external pressures: children leaving home, caring for ageing parents, and shifting relationship dynamics. Marino notes that "the emotional and physical stress that often accompanies these changes can lead to changes in eating habits and weight gain." Chronic stress elevates cortisol, a hormone strongly linked to abdominal fat accumulation.

Could Your Medication Be Contributing?
This is a factor that often goes unexamined: certain medications commonly prescribed during menopause can promote weight gain. These include:
- SNRIs and SSRIs — used to treat depression and anxiety, and sometimes prescribed for hot flashes
- Gabapentin — prescribed for hot flashes and nerve pain
- Beta blockers — used to manage high blood pressure and heart-related symptoms
If you've started a new medication and noticed weight changes, it's worth raising with your prescriber. Marino advises women to ask specifically about alternate medications that treat the same condition without weight gain as a side effect. Sometimes a substitution is possible; sometimes it isn't — but the conversation is worth having.
Why Menopause Belly Fat Is a Health Risk, Not Just a Cosmetic Issue
One of the most important — and least discussed — aspects of menopause belly fat is what type of fat it actually is. During menopause, subcutaneous fat (the fat stored just beneath the skin) has a tendency to convert to visceral fat. Visceral fat sits deep within the abdominal cavity, surrounding organs like the liver, stomach, and intestines.
Unlike subcutaneous fat, visceral fat is metabolically active in harmful ways. It is directly linked to:
- Cardiovascular disease
- Type 2 diabetes (via insulin resistance)
- Certain types of cancer
The good news is that even modest weight loss reduces visceral fat significantly. Research cited by Marino suggests that losing just 5–10% of body weight can measurably improve your metabolic profile and reduce disease risk. You don't need to aim for dramatic transformation — meaningful health gains are achievable.

How to Fight Menopause Belly Fat: Evidence-Based Strategies
"There is no magic way to lose belly fat," says Marino. "It really comes down to the basics of diet and exercise." That said, the specifics matter — and menopause changes what "the basics" should look like.
Adjust Your Diet for a Slower Metabolism
Metabolism slows during menopause, meaning the calorie intake that kept your weight stable at 35 may now contribute to gradual gain. Reducing overall calorie intake is necessary, but what you eat matters as much as how much.
Marino recommends a diet that is largely plant-based and low in processed foods and saturated fat. This approach reduces visceral fat accumulation, supports cardiovascular health, and provides the fibre needed to keep hunger hormones in check. Simple carbohydrates — the foods most often craved when tired or stressed — are the biggest dietary driver of abdominal fat and should be minimised.
Combine Aerobic Exercise With Strength Training
Increased physical activity paired with a calorie reduction is the most effective formula for weight loss at any age — but for menopausal women, the type of exercise matters. Aerobic exercise (walking, cycling, swimming) supports heart health and burns calories. Resistance or weight training builds lean muscle mass, which boosts resting metabolism and protects bone density — both of which decline during menopause.
Aiming for a combination of both, rather than focusing solely on cardio, produces better body composition outcomes and longer-term health benefits.
Consider Menopause Hormone Therapy (MHT)
A common misconception is that hormone therapy causes weight gain — the evidence says otherwise. Marino is clear: "Menopause hormone therapy (MHT) does not cause weight gain and can, in an indirect way, help with weight loss."
MHT works indirectly by addressing the root conditions that drive weight gain: improving sleep quality, increasing energy levels, reducing joint pain, and stabilising mood. Women who sleep better and feel better are more likely to exercise and make healthier food choices. Candidates most likely to benefit are women who are perimenopausal, within 10 years of their last menstrual period, or younger than 60 — though individual medical history always applies.
Manage Stress Actively
Stress management isn't a soft recommendation — it's a direct intervention against visceral fat accumulation. Chronic elevated cortisol is a well-documented driver of abdominal fat, and addressing it requires deliberate effort. Effective approaches include:
- Nutrition — reducing sugar and caffeine, which amplify stress responses
- Exercise — a proven cortisol regulator
- Integrative therapies — acupuncture, meditation, yoga, and massage therapy all have evidence supporting stress reduction
- Behavioural health counselling — particularly useful for women dealing with significant life transitions alongside hormonal change
Medical and Surgical Options
For women with significant risk factors for weight-related illness, bariatric surgery or prescription weight-loss medications may be appropriate options to discuss with a healthcare provider. These are not first-line approaches, but they are legitimate and increasingly accessible tools when lifestyle interventions alone are insufficient.

The Bottom Line on Menopause Belly Fat
Menopause belly fat is real, it's common, and it has multiple overlapping causes — hormonal shifts, sleep disruption, stress, medication side effects, and reduced activity. Understanding which factors are driving your individual experience is the starting point for addressing it effectively.
The strategies with the strongest evidence are consistent: move more, eat a whole-food plant-based diet, address sleep problems, manage stress, and explore whether hormone therapy is appropriate for you. Losing even 5–10% of body weight can shift your metabolic risk profile meaningfully.
Perhaps most importantly, remember that body changes during menopause are a normal part of ageing — not a personal failure. As Marino puts it: "Women can be really hard on themselves... try to show yourself a little love and compassion during this new stage of life."